|
|
市場調査レポート
商品コード
1376843
非転移性前立腺がん(nmPC)市場 - 市場の洞察、疫学、市場予測:2032年Non-metastatic Prostate Cancer (nmPC) - Market Insight, Epidemiology and Market Forecast -2032 |
||||||
|
|
|||||||
カスタマイズ可能
|
|||||||
| 非転移性前立腺がん(nmPC)市場 - 市場の洞察、疫学、市場予測:2032年 |
|
出版日: 2023年11月01日
発行: DelveInsight
ページ情報: 英文 200 Pages
納期: 1~3営業日
|

全表示
- 概要
- 図表
- 目次
非転移性前立腺がん(nmPC)とは、前立腺とその近傍のリンパ節を超えて転移していない前立腺がんを指します。前立腺がんの限局型です。前立腺がんがこの病期で診断されるということは、がん細胞が前立腺に限局しており、周囲の組織への浸潤や骨、肺、肝臓などの遠隔臓器への転移(拡がり)をまだ起こしていないことを意味します。
非転移性前立腺がんは通常、前立腺特異抗原(PSA)血液検査、直腸指診(DRE)、前立腺生検などの検査を組み合わせて診断されます。また、前立腺内のがんの範囲や位置を評価するために、マルチパラメトリック磁気共鳴画像法(mpMRI)などの画像診断法を用いることもあります。
前立腺がんの病期分類は、疾患の範囲を決定するのに役立ちます。非転移性前立腺がんは通常、腫瘍の大きさ、近傍構造物への浸潤、リンパ節転移などの因子別、i期、II期、III期に分類されます。がんは前立腺およびその近傍に限局していると考えられます。
非転移性前立腺がんに対する治療法の選択は、患者さんの年齢、全身の健康状態、がんの侵攻性、個人の嗜好など、さまざまな要因別異なります。治療法には、積極的監視療法、手術療法、放射線療法、ホルモン療法などがあります。
主要7ヶ国地域では、米国が2022年に最大の市場規模を獲得しています。2022年、米国は32億米ドルを占めています。主要7ヶ国諸国の中で最も市場規模が小さいのはスペインで、1億5,000万米ドルです。初期治療に関しては、2022年の市場規模は手術が最も大きく、13億米ドルです。
当レポートでは、主要7ヶ国における非転移性前立腺がん(nmPC)市場について調査し、市場の概要とともに、疫学、患者動向、新たな治療法、2032年までの市場規模予測、および医療のアンメットニーズなどを提供しています。
目次
第1章 重要な洞察
第2章 レポートのイントロダクション
第3章 非転移性前立腺がん市場概要
第4章 非転移性前立腺がんのエグゼクティブサマリー
第5章 主要な出来事
第6章 疾患の背景と概要
第7章 治療と管理
第8章 疫学と患者数
- 主な調査結果
- 仮定と根拠
- 主要7ヶ国における非転移性前立腺がんの有病者数の合計
- 米国における疫学シナリオ
- EU4ヶ国と英国における疫学シナリオ
- 日本における疫学シナリオ
第9章 患者動向
第10章 上市済み薬剤
第11章 新興の治療法
第12章 非転移性前立腺がん:主要7ヶ国市場分析
- 主な調査結果
- 市場の見通し
- コンジョイント分析
- 主要な市場予測の前提条件
- 主要7ヶ国の市場規模
- 米国の市場規模
- EU4ヶ国と英国の市場規模
- 日本の市場規模
第13章 KOLのビュー
第14章 SWOT分析
第15章 アンメットニーズ
第16章 市場アクセスと償還
第17章 付録
第18章 DelveInsightのサービス内容
第19章 免責事項
第20章 DelveInsightについて
List of Tables
- Table 1: Summary of Non-metastatic Prostate Cancer, Market, Epidemiology, and Key Events (2019-2032)
- Table 2: Total Diagnosed Prevalent Cases of Prostate Cancer in the 7MM
- Table 3: Total Diagnosed Prevalent Cases of Non-metatstatic Prostate Cancer in the 7MM
- Table 4: Total Diagnosed Prevalent Cases of Prostate Cancer in the United States
- Table 5: Total Age-specific Cases of Prostate Cancer in the United States
- Table 6: Total Stage-specific Cases of Prostate Cancer in the United States
- Table 7: Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in the United States
- Table 8: Total Diagnosed Prevalent Cases of Prostate Cancer in EU4 and the UK
- Table 9: Total Age-specific Cases of Prostate Cancer in EU4 and the UK
- Table 10: Total Stage-specific Cases of Prostate Cancer in EU4 and the UK
- Table 11: Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in EU4 and the UK
- Table 12: Total Diagnosed Prevalent Cases of Prostate Cancer in Japan
- Table 13: Total Age-specific Cases of Prostate Cancer in Japan
- Table 14: Total Stage-specific Cases of Prostate Cancer in Japan
- Table 15: Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in Japan
- Table 16: ORGOVYX (relugolix), Clinical Trial Description, 2023
- Table 17: CAN-2409, Clinical Trial Description, 2023
- Table 18: Total Market Size of Non-metastatic Prostate Cancer in the 7MM
- Table 19: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in the 7MM
- Table 20: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in the 7MM
- Table 21: Market Size of nmCRPC by Therapies in the 7MM
- Table 22: Total Market Size of Non-metastatic Prostate Cancer in the United States
- Table 23: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in the United States
- Table 24: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in the United States
- Table 25: Market Size of nmCRPC by Therapies in the United States
- Table 26: Total Market Size of Non-metastatic Prostate Cancer in EU4 and the UK
- Table 27: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in EU4 and the UK
- Table 28: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in EU4 and the UK
- Table 29: Market Size of nmCRPC by Therapies in EU4 and the UK
- Table 30: Total Market Size of Non-metastatic Prostate Cancer in Japan
- Table 31: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in Japan
- Table 32: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in Japan
- Table 33: Market Size of nmCRPC by Therapies in Japan
List of Figures
- Figure 1: Summary of Non-metastatic Prostate Cancer, Market, Epidemiology, and Key Events (2019-2032)
- Figure 2: Total Diagnosed Prevalent Cases of Prostate Cancer in the 7MM
- Figure 3: Total Diagnosed Prevalent Cases of Non-metatstatic Prostate Cancer in the 7MM
- Figure 4: Total Diagnosed Prevalent Cases of Prostate Cancer in the United States
- Figure 5: Total Age-specific Cases of Prostate Cancer in the United States
- Figure 6: Total Stage-specific Cases of Prostate Cancer in the United States
- Figure 7: Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in the United States
- Figure 8: Total Diagnosed Prevalent Cases of Prostate Cancer in EU4 and the UK
- Figure 9: Total Age-specific Cases of Prostate Cancer in EU4 and the UK
- Figure 10: Total Stage-specific Cases of Prostate Cancer in EU4 and the UK
- Figure 11: Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in EU4 and the UK
- Figure 12: Total Diagnosed Prevalent Cases of Prostate Cancer in Japan
- Figure 13: Total Age-specific Cases of Prostate Cancer in Japan
- Figure 14: Total Stage-specific Cases of Prostate Cancer in Japan
- Figure 15: Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in Japan
- Figure 16: ORGOVYX (relugolix), Clinical Trial Description, 2023
- Figure 17: CAN-2409, Clinical Trial Description, 2023
- Figure 18: Total Market Size of Non-metastatic Prostate Cancer in the 7MM
- Figure 19: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in the 7MM
- Figure 20: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in the 7MM
- Figure 21: Market Size of nmCRPC by Therapies in the 7MM
- Figure 22: Total Market Size of Non-metastatic Prostate Cancer in the United States
- Figure 23: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in the United States
- Figure 24: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in the United States
- Figure 25: Market Size of nmCRPC by Therapies in the United States
- Figure 26: Total Market Size of Non-metastatic Prostate Cancer in EU4 and the UK
- Figure 27: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in EU4 and the UK
- Figure 28: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in EU4 and the UK
- Figure 29: Market Size of nmCRPC by Therapies in EU4 and the UK
- Figure 30: Total Market Size of Non-metastatic Prostate Cancer in Japan
- Figure 31: Market Size of Non-metastatic Prostate Cancer by Initial Therapies in Japan
- Figure 32: Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in Japan
- Figure 33: Market Size of nmCRPC by Therapies in Japan
- Figure 34: Unmet Needs
Key Highlights:
- Non-metastatic prostate cancer (nmPC) refers to prostate cancer that has not spread beyond the prostate gland and nearby lymph nodes. It is a localized form of prostate cancer. When prostate cancer is diagnosed at this stage, it means that cancer cells are confined to the prostate and have not yet invaded surrounding tissues or metastasized (spread) to distant organs, such as bones, lungs, or liver.
- Non-metastatic Prostate Cancer is typically diagnosed through a combination of tests, including prostate-specific antigen (PSA) blood tests, digital rectal exams (DRE), and prostate biopsies. Imaging techniques, such as multiparametric magnetic resonance imaging (mpMRI), may also be used to assess the extent and location of the cancer within the prostate.
- The staging of prostate cancer helps determine the extent of the disease. Non-metastatic prostate cancer is typically categorized as stage I, stage II, or stage III, depending on factors like tumor size, involvement of nearby structures, and lymph node involvement. The cancer is considered localized within the prostate and nearby areas.
- The choice of treatment for non-metastatic Prostate Cancer depends on various factors, including the patient's age, overall health, the aggressiveness of the cancer, and individual preferences. The treatment options include active surveillance, surgery, radiation therapy as well as hormone therapy.
- While non-metastatic Prostate Cancer is localized, there is always a risk that it may progress to a more advanced stage, including metastatic prostate cancer. The goal of treatment and monitoring is to delay or prevent such progression.
- Ongoing research and clinical trials aim to improve treatments for non-metastatic Prostate Cancer and may offer patients access to innovative therapies and treatment strategies.
- The approved treatment options for non-metastatic prostate cancer include XTANDI, ERLEADA and NUBEQA.
Report Summary:
- The detailed report provides significant knowledge about epidemiological segments including the historical as well as forecasted patient pool data, thus providing a thorough picture of anticipated future development in diagnostic rates, disease progression, and treatment guidelines. It gives deep insights into various areas, allowing for a complete examination of the subject.
- The report also includes an all-inclusive account of current management techniques and emerging therapies, as well as elaborative profiles of late-stage (Phase III and Phase II) and prominent therapies that would impact the current treatment landscape and result in an overall market shift. The therapy profiles include detailed assessment of the current and emerging therapies including information regarding the approval-based as well as ongoing trials along with thorough drug description. The report also includes surgery data as well. Detailed account of different surgical procedures has been provided in the report.
- The report also encompasses a comprehensive analysis of Non-metastatic Prostate Cancer market, providing an in-depth examination of its historical and projected market size (2019-2032). It also includes the market share of therapies, along with detailed assumptions and the underlying rationale for our methodology. The report also includes drug outreach coverage in the 7MM region.
- The report includes qualitative as well as quantitative insights that provide an edge while developing business strategies, by understanding trends, through SWOT analysis and expert insights/KOL views, including experts from various hospitals and prominent universities, patient journey which gives an overview of the patient landscape commencing from detection of the disease to treatment being administered to the patients, with the treatment preferences that help shape and drive the 7MM Non-metastatic Prostate Cancer market.
Market
There are various key players currently investigating their drugs for Non-metastatic Prostate Cancer, such as Myovant Sciences, Kangpu Biopharmaceuticals, and Candel Therapeutics etc. The details of the country and therapy-wise market size have been provided below.
- In the 7MM region, the United States was found to capture the largest market size in 2022. In 2022, the United States accounted for ~USD 3,200 million
- Among the 7MM countries, Spain accounted for the smallest market size that is ~USD 150 million.
- As far as the initial therapies are concerned, surgery accounted for the highest market size in 2022 that is ~ USD 1,300 million.
- Among the therapies given to biochemical recurrence patients, systemic therapy garnered the largest market size that is around USD 260 million.
Non-metastatic Prostate Cancer Drug Chapters
The Non-metastatic Prostate Cancer report's drugs section includes an in-depth examination of marketed drugs as well as late-stage pipeline therapeutics (Phase III and Phase II) for Non-metastatic Prostate Cancer.
The drug chapters section contains useful information on various aspects of Non-metastatic Prostate Cancer clinical trials, including specific details such as the pharmacological mechanisms of the drugs involved, designations, approval status, patent information, and a comprehensive analysis of the pros and cons associated with each drug. It also includes the most recent news updates and press releases on drugs that treat Non-metastatic Prostate Cancer.
Marketed Therapies
ERLEADA (apalutamide): Janssen Pharmaceutical
ERLEADA (apalutamide) is a next-generation oral AR inhibitor that blocks the androgen signaling pathway in prostate cancer cells. It is indicated for the treatment of patients with nmCRPC and with mCSPC. It is taken orally, once daily, with or without food. ERLEADA inhibits the growth of cancer cells in three ways: by preventing the binding of androgen to the AR, by stopping the AR from entering the cancer cells, and by preventing the AR from binding to the DNA of the cancer cell.
ORGOVYX (relugolix): Myovant Sciences
ORGOVYX (relugolix) is an oral gonadotropin-releasing hormone (GnRH) receptor antagonist approved by the FDA for treating adult patients with advanced prostate cancer. As a GnRH antagonist, ORGOVYX blocks the GnRH receptor and reduces the production of testicular testosterone, a hormone known to stimulate the growth of prostate cancer. Relugolix is a nonpeptide GnRH receptor antagonist that competitively binds to pituitary GnRH receptors, thereby reducing the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) and, consequently, testosterone
Note: Detailed assessment will be provided in the final report of Non-metastatic Prostate Cancer…
Emerging Therapies
CAN-2409: Candel Therapeutics
CAN-2409, Candel's most advanced viral immunotherapy candidate, is a replication-defective adenovirus that delivers the herpes simplex virus thymidine kinase (HSV-tk) gene to cancer cells. HSV-tk is an enzyme that locally converts orally administered valacyclovir into a toxic metabolite that kills nearby cancer cells. The intra-tumoral administration results in the release of tumor-specific neoantigens in the microenvironment. At the same time, the adenoviral serotype 5 capsid protein elicits a strong pro-inflammatory signal in the tumor microenvironment, which is designed to create the optimal conditions to induce an individualized and specific CD8+ T cell-mediated response against the injected tumor and uninjected distant metastases for broad anti-tumor
Note: Detailed assessment will be provided in the final report of Non-metastatic Prostate Cancer…
Non-metastatic Prostate Cancer Market Outlook
Non-metastatic castration-sensitive prostate cancer is abbreviated as nmCSPC. It essentially refers to prostate cancer that has not migrated to other regions of the body and remains responsive to hormone treatment (ADT). The prevalence of mCSPC, the availability of effective therapies, evolving treatment recommendations, and the pharmaceutical sector's investment in research and development all have an impact on the market potential for nmCSPC.
With the development of cutting-edge drugs such as androgen receptor inhibitors (ARIs) such as ERLEADA (apalutamide), XTANDI (enzalutamide), and NUBEQA (darolutamide), the therapeutic landscape for nmCSPC has changed substantially. The approval of these drugs have broadened treatment choices beyond standard hormone therapy.
The traditional therapeutic method for nmCRPC patients, androgen deprivation therapy (ADT) alone until metastatic disease, is now thought to be inadequate. Several randomised Phase III clinical studies have shown considerable clinical advantages for therapies that combine ADT with apalutamide, enzalutamide, and darolutamide, including considerably improved overall survival (OS).
Metastasis-free survival (MFS) improvement in the PROSPER, SPARTAN, and ARAMIS studies supports the use of enzalutamide, apalutamide, and darolutamide in patients with nmCRPC. Because there have been no direct clinical trials comparing these three therapies, no single therapy can be established to be the best therapy in terms of clinical effectiveness or safety. In comparison to the placebo, each of these drugs has exhibited a fair safety and adverse event profile.
According to research presented at the ASCO Genitourinary Cancers Symposium (2023), it was found that patients with nmCRPC treated with NUBEQA (darolutamide) were less likely to develop metastatic disease or discontinue treatment due to adverse events than patients treated with XTANDI (enzalutamide) or ERLEADA (apalutamide).
Note: Detailed assessment will be provided in the final report of Non-metastatic Prostate Cancer…
Non-metastatic Prostate Cancer Understanding and Treatment
Non-metastatic Prostate Cancer Overview
Non-metastatic prostate cancer refers to prostate cancer that has not spread beyond the prostate gland and nearby lymph nodes. It is a localized form of prostate cancer. Prostate cancer is a highly endocrine-responsive disease. It re-lies profoundly on the androgen signaling pathway for its growth and survival.
Prostate cancer occurs when the DNA in cells in the prostate develops mutations that may disable their ability to control cell growth and division. In many cases, these mutated cells die or are attacked by the immune system. However, some mutated cells may escape the immune system and grow out of control, forming a prostate tumor
Detailed overview will be provided in the final report…
Non-metastatic Prostate Cancer Diagnosis
Screening is testing to find cancer in people before they have symptoms. However, It is unclear if the benefits of prostate cancer screening outweigh the risks for most men. Still, after discussing the pros and cons of screening with their doctors, some men might reasonably choose to be screened. If one of these test results is abnormal, patients will probably need a prostate biopsy to know the cancer occurrence.
Further details related to diagnosis are provided in the report…
Non-metastatic Prostate Cancer Treatment
Localized prostate cancer represents a paradox when left untreated; it is generally associated with a good prognosis. However, because prostate cancer is a common cause of cancer-related mortality, there is usually significant patient anxiety once the diagnosis is confirmed. All standard treatments carry risks of adverse events that might negatively impact short-, medium-, or long-term quality of life. As such, the clinical approach to managing localized prostate cancer must consider not only the disease features, such as stage, grade, and volume of cancer detected, but also patient comorbidities, life expectancy, and priorities.
The optimal management of localized prostate cancer starts with discussion by a multidisciplinary team (MDT) consisting of radiation oncologists, medical oncologists, urologists, histopathologists, radiologists, and specialist nurses. Each brings their expertise and knowledge of the patient to help determine which treatment options are appropriate for an individual.
Further details related to treatment and management are provided in the report…..
Non-metastatic Prostate Cancer Epidemiology
The Non-metastatic Prostate Cancer epidemiology chapter in the report provides historical as well as forecasted epidemiology segmented by, Total Diagnosed Prevalent Cases of Non-metastatic Prostate Cancer, Total Age-specific Cases of Non-metastatic Prostate Cancer, Total Stage-specific Cases of Non-metastatic Prostate Cancer, Total Line-wise Treated Cases of Non-metastatic Prostate Cancer covering the United States, EU4 countries (Germany, France, Italy, Spain) and the United Kingdom, and Japan from 2019 to 2032.
- The total diagnosed prevalent cases of prostate cancer in the United States were ~1,409,000 in 2022. The cases are expected to increase by 2032.
- In Japan, the highest number of cases of prostate cancer were found in the 65-74 years age group. The least number of patients belonged to the = 54 years age group.
- The total stage-specific cases of prostate cancer in EU4 and the UK in 2022 were ~7,002,000 and ~490,000 cases for locally advanced (Stage I-III) and metastatic stage (Stage IV), respectively
Further details related to epidemiology will be provided in the report…
KOL Views
In order to stay abreast of the latest trends in the market, we conduct primary research by seeking the opinions of Key Opinion Leaders (KOLs) and Subject Matter Experts (SMEs) who work in the relevant field. This helps us fill any gaps in data and validate our secondary research.
We have reached out to industry experts to gather insights on various aspects of Non-metastatic Prostate Cancer, including the evolving treatment landscape, patients' reliance on conventional therapies, their acceptance of therapy switching, drug uptake, and challenges related to accessibility. The experts included medical/scientific writers, professors, and researchers from prestigious universities in the US, Europe, the UK, and Japan.
Our team of analysts at DelveInsight connected with more than 10 KOLs across the 7 Major Markets (7MM). We contacted institutions such as Duke University, University of Manchester, and others. By obtaining the opinions of these experts, we gained a better understanding of the current and emerging treatment patterns in the Non-metastatic Prostate Cancer market, which will assist our clients in analyzing the overall epidemiology and market scenario.
Qualitative Analysis
We conduct qualitative and market intelligence analysis employing a variety of methods, including SWOT analysis and Conjoint Analysis. Strengths, weaknesses, opportunities, and threats in disease diagnosis, patient awareness, patient burden, competitive landscape, cost-effectiveness, and geographical accessibility of therapies are described in the SWOT analysis. These recommendations are based on the Analyst's evaluation of the patient burden, cost analysis, and the current and emerging therapy landscape. Conjoint Analysis compares the effectiveness and safety of numerous approved and emergent drugs depending on key criteria such as frequency of administration, designation, route of administration, and order of entry. To assess the success of therapy, several factors are evaluated.
Furthermore, the drug's safety is analyzed, in which acceptability, tolerability, and adverse events are closely monitored, and it establishes a firm grasp of the side effects posed by the drugs used in the trials. Furthermore, for each therapy, the rating is based on the route of administration, sequence of entrance and designation, chance of success, and addressable patient pool. The ultimate weightage score and ranking of developing therapeutics are determined by these characteristics.
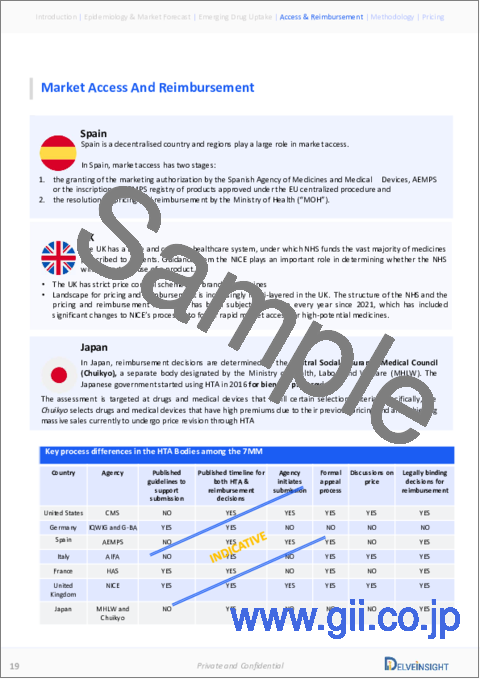
Market Access and Reimbursement
Because newly authorized drugs are often expensive, some patients escape receiving proper treatment or use off-label, less expensive prescriptions. Reimbursement plays a critical role in how innovative treatments can enter the market. The cost of the medicine, compared to the benefit it provides to patients who are being treated, sometimes determines whether or not it will be reimbursed. Regulatory status, target population size, the setting of treatment, unmet needs, the number of incremental benefit claims, and prices can all affect market access and reimbursement possibilities.
The report further provides detailed insights on the country-wise accessibility and reimbursement scenarios, cost-effectiveness scenario of approved therapies, programs making accessibility easier and out-of-pocket costs more affordable, insights on patients insured under federal or state government prescription drug programs, etc.
Non-metastatic Prostate Cancer Report Insights
- Patient Population
- Therapeutic Approaches
- Line-wise market size of therapies
- Non-metastatic Prostate Cancer Market Size and Trends
- Existing Market Opportunity
Non-metastatic Prostate Cancer Report Key Strengths
- Ten-year Forecast
- The 7MM Coverage
- Non-metastatic Prostate Cancer Epidemiology Segmentation (Segmented by age and stage-specific cases and line-wise treated cases)
- Key Cross Competition evaluating the marketed as well as emerging therapies
Non-metastatic Prostate Cancer Report Assessment
- Current Treatment and Management Practices
- Unmet Needs
- Market Attractiveness
- Qualitative Analysis (SWOT, Conjoint Analysis)
Key Questions
- Would there be any changes observed in the current treatment approach?
- Will there be any improvements in Non-metastatic Prostate Cancer management recommendations?
- Would research and development advances pave the way for future tests and therapies for Non-metastatic Prostate Cancer?
- Would the innovations in diagnostic tests of Non-metastatic Prostate Cancer space experience a significant impact and lead to a positive shift in the treatment landscape of Non-metastatic Prostate Cancer?
- What kind of uptake the new therapies are going to witness in the coming years in Non-metastatic Prostate Cancer patients?
Table of Contents
1. Key Insights
2. Report Introduction
3. Non-metastatic Prostate Cancer Market Overview at a Glance
- 3.1. Market Share (%) Distribution of Non-metastatic Prostate Cancer in 2019
- 3.2. Market Share (%) Distribution of Non-metastatic Prostate Cancer in 2032
4. Executive Summary of Non-metastatic Prostate Cancer
5. Key Events
6. Disease Background and Overview
- 6.1. Disease Background and Overview
- 6.2. Signs and Symptoms of Prostate Cancer
- 6.3. Early Symptoms of Prostate Cancer
- 6.4. Advanced Prostate Cancer Symptoms
- 6.5. Recurrent Prostate Cancer Symptoms
- 6.6. Risk Factors and Causes of Prostate Cancer
- 6.7. Pathophysiology of Prostate Cancer
7. Treatment and Management
8. Epidemiology and Patient Population
- 8.1. Key Findings
- 8.2. Assumption and Rationale
- 8.3. Total Prevalent Cases of Non-metastatic Prostate Cancer in the 7MM
- 8.4. Epidemiology Scenario in the United States
- 8.4.1. Total Diagnosed Prevalent Cases of Prostate Cancer in the United States
- 8.4.2. Total Age-specific Cases of Prostate Cancer in the United States
- 8.4.3. Total Stage-specific Cases of Prostate Cancer in the United States
- 8.4.4. Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in the United States
- 8.5. Epidemiology Scenario in EU4 and the UK
- 8.5.1. Total Diagnosed Prevalent Cases of Prostate Cancer in EU4 and the UK
- 8.5.2. Total Age-specific Cases of Prostate Cancer in EU4 and the UK
- 8.5.3. Total Stage-specific Cases of Prostate Cancer in EU4 and the UK
- 8.5.4. Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in EU4 and the UK
- 8.6. Epidemiology Scenario in Japan
- 8.6.1. Total Diagnosed Prevalent Cases of Prostate Cancer in Japan
- 8.6.2. Total Age-specific Cases of Prostate Cancer in Japan
- 8.6.3. Total Stage-specific Cases of Prostate Cancer in Japan
- 8.6.4. Total Line-wise Treated Cases of Non-metastatic Prostate Cancer in Japan
9. Patient Journey
10. Marketed Therapies
- 10.1. Key Cross Competition: Marketed Therapies
- 10.2. ERLEADA (apalutamide): Janssen Pharmaceutical
- 10.2.1. Product Description
- 10.2.2. Regulatory Milestones
- 10.2.3. Other Development Activities
- 10.2.4. Clinical Development Activities
- 10.2.5. Safety and Efficacy
- To be continued in the report…
11. Emerging Therapies
- 11.1. Key Cross Competition: Emerging Therapies
- 11.2. CAN-2409: Candel Therapeutics
- 11.2.1. Product Description
- 11.2.2. Other Development Activities
- 11.2.3. Clinical Development Activities
- 11.2.4. Safety and Efficacy
- To be continued in the report…
12. Non-metastatic Prostate Cancer: 7 Major Market Analysis
- 12.1. Key Findings
- 12.2. Market Outlook
- 12.3. Conjoint Analysis
- 12.4. Key Market Forecast Assumptions
- 12.5. 7MM Market Size
- 12.5.1. Total Market Size of Non-metastatic Prostate Cancer in the 7MM
- 12.5.2. Market Size of Non-metastatic Prostate Cancer by Initial Therapies in the 7MM
- 12.5.3. Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in the 7MM
- 12.5.4. Market Size of nmCRPC by Therapies in the 7MM
- 12.6. United States Market Size
- 12.6.1. Total Market Size of Non-metastatic Prostate Cancer in the United States
- 12.6.2. Market Size of Non-metastatic Prostate Cancer by Initial Therapies in the United States
- 12.6.3. Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in the United States
- 12.6.4. Market Size of nmCRPC by Therapies in the United States
- 12.7. EU4 and the UK Market Size
- 12.7.1. Total Market Size of Non-metastatic Prostate Cancer in EU4 and the UK
- 12.7.2. Market Size of Non-metastatic Prostate Cancer by Initial Therapies in EU4 and the UK
- 12.7.3. Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in EU4 and the UK
- 12.7.4. Market Size of nmCRPC by Therapies in EU4 and the UK
- 12.8. Japan Market Size
- 12.8.1. Total Market Size of Non-metastatic Prostate Cancer in Japan
- 12.8.2. Market Size of Non-metastatic Prostate Cancer by Initial Therapies in Japan
- 12.8.3. Market Size of Non-metastatic Prostate Cancer by Biochemical Recurrence Therapies in Japan
- 12.8.4. Market Size of nmCRPC by Therapies in Japan
13. KOL Views
14. SWOT Analysis
15. Unmet Needs
16. Market Access and Reimbursement
- 16.1. Reimbursement
- 16.2. Key HTA Decisions
- 16.3. Patient Access Program
17. Appendix
- 17.1. Bibliography
- 17.2. Report Methodology
- 17.3. Acronyms and Abbreviations